
Expert Fever & Tropical
Infection Care in Surat
Fever is a signal — not a diagnosis. In Surat during monsoon, the same fever can be dengue, malaria, typhoid, chikungunya, or viral illness — each requiring completely different treatment. Dr. Pratik Savaj identifies the cause with the right test, on the right day, before the wrong treatment causes harm.
Fever Is a Signal — Not a Diagnosis. The Cause Is What Matters.
Every fever is the body raising its core temperature to fight an infection or inflammatory process. The fever itself is not the problem — the underlying cause is. The most dangerous clinical error in Surat is treating the fever without identifying what is causing it. Giving ibuprofen to a dengue patient causes bleeding. Giving ciprofloxacin to a fluoroquinolone-resistant typhoid patient fails. Treating “viral fever” when the patient actually has TB delays a curable diagnosis by months.
In Surat during monsoon from July to November, the same presenting fever could be dengue (Aedes mosquito), malaria (Anopheles mosquito), typhoid (contaminated water), chikungunya (Aedes mosquito), leptospirosis (flood water), scrub typhus (mite bite), or viral illness. Each requires a different diagnostic test, on a different day, with different treatment implications. This is exactly the clinical complexity that an infectious disease specialist is trained for.
At IID Hospital, Dr. Savaj’s approach to fever is systematic: the right test on the right day, before starting the right treatment. Not empirical prescribing. Not the same antibiotic for every fever. Diagnosis first.

Dr. Pratik Savaj
FNB Infectious Diseases · IID Hospital, Surat
Fever & tropical infection specialist
Test Before Treating
NS1 antigen on day 1 for dengue. Blood smear + RDT on day 1 for malaria. Blood culture before starting antibiotics for suspected typhoid. One missed test on day 1 can mean a wrong treatment, a delayed diagnosis, and a preventable complication.
No NSAIDs Until Dengue Excluded
Ibuprofen and aspirin inhibit platelet function. In dengue, where platelets are already falling, NSAIDs cause dangerous bleeding. Paracetamol only for all fever in Surat during monsoon until dengue NS1 is formally negative.
Never Assume “Just Viral”
During Surat monsoon (July–November), never assume fever is viral without excluding dengue and malaria first. Both begin as undifferentiated fever. Dengue can be fatal if missed at the critical phase. Malaria can cause cerebral involvement within days.
Symptoms That Warrant a Specialist Consultation
Different fevers in Surat produce overlapping symptoms in the first 24–48 hours — but each infection has characteristic features that develop over days. Knowing which symptom pattern to watch for determines which test to order, on which day, and whether a patient is in the safe zone or the danger zone.
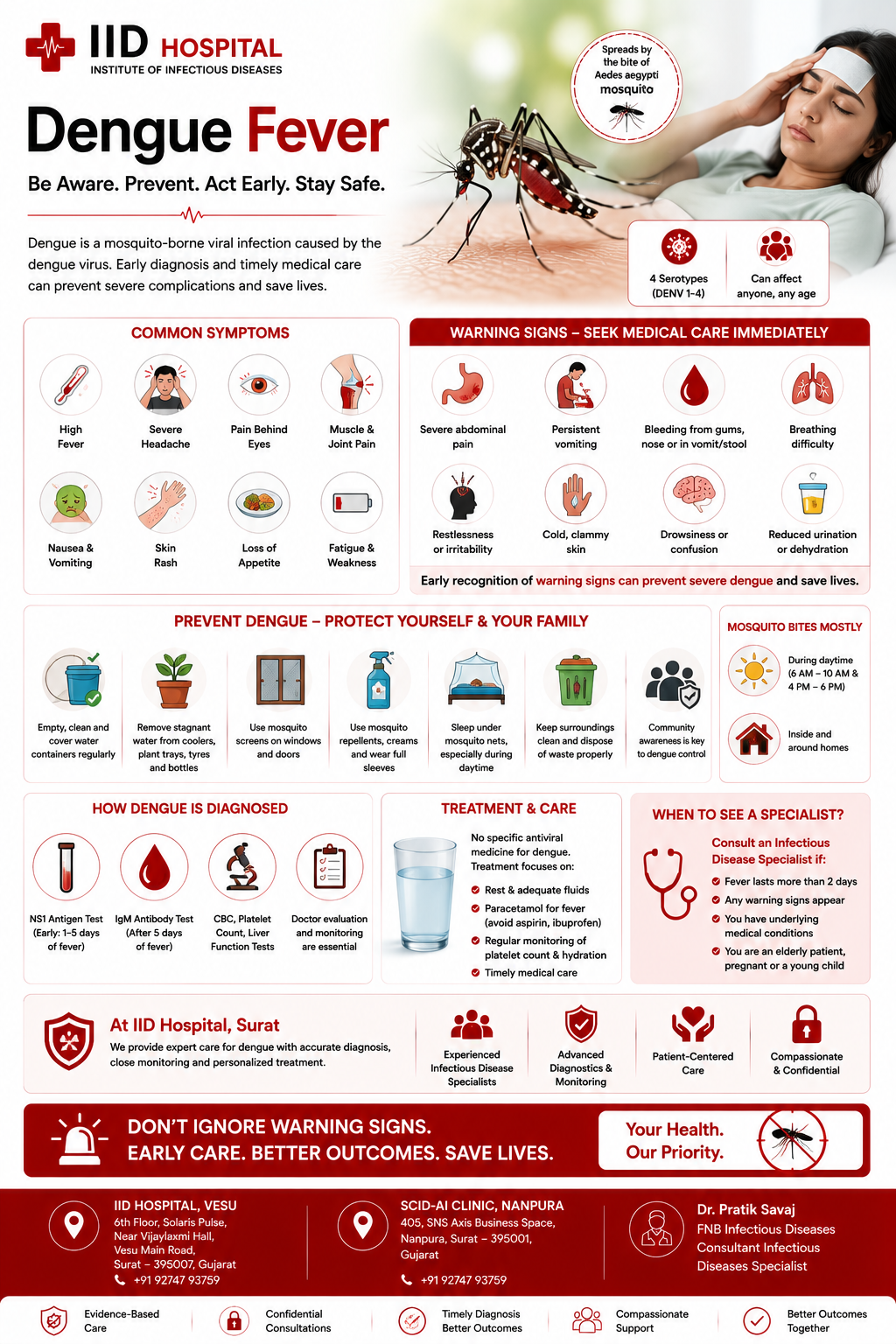
Dengue Warning Signs
These are severe dengue warning signs — go to emergency immediately.
Malaria Warning Signs
Falciparum malaria can cause cerebral involvement within 24–48 hours. Test and treat urgently.
Typhoid Warning Signs
Sudden severe abdominal pain in typhoid = possible intestinal perforation. Emergency.
Chikungunya Signs
Post-chikungunya arthritis needs hydroxychloroquine — not just paracetamol and waiting.
Leptospirosis & Scrub Typhus
Always check for eschar in FUO. Often hidden. Look carefully at axilla, groin, and scalp.
See Dr. Savaj Urgently
+91 92747 93759 — Call or WhatsApp Dr. Savaj, IID Hospital, Surat.
The Paracetamol Rule
During Surat monsoon (July–November): use only paracetamol for fever management until dengue has been formally excluded by negative NS1 antigen test.
Never use ibuprofen or aspirin for monsoon fever — both inhibit platelet function and can cause severe bleeding if the fever is dengue.
Temperature Monitoring
Every Tropical Fever — Managed With Specialist Depth
IID Hospital manages the full spectrum of fever and tropical infection in Surat. Each condition requires a different diagnostic test on a different day, a different treatment, and carries different risks if missed or mismanaged.
Dengue Fever
The most dangerous monsoon fever in Surat. The critical phase (days 4–6) — when fever drops but plasma leaks — is where patients deteriorate if not monitored. Daily platelet count monitoring during the critical phase is the standard of care at IID Hospital, not optional.
Symptoms
IID Hospital Protocol
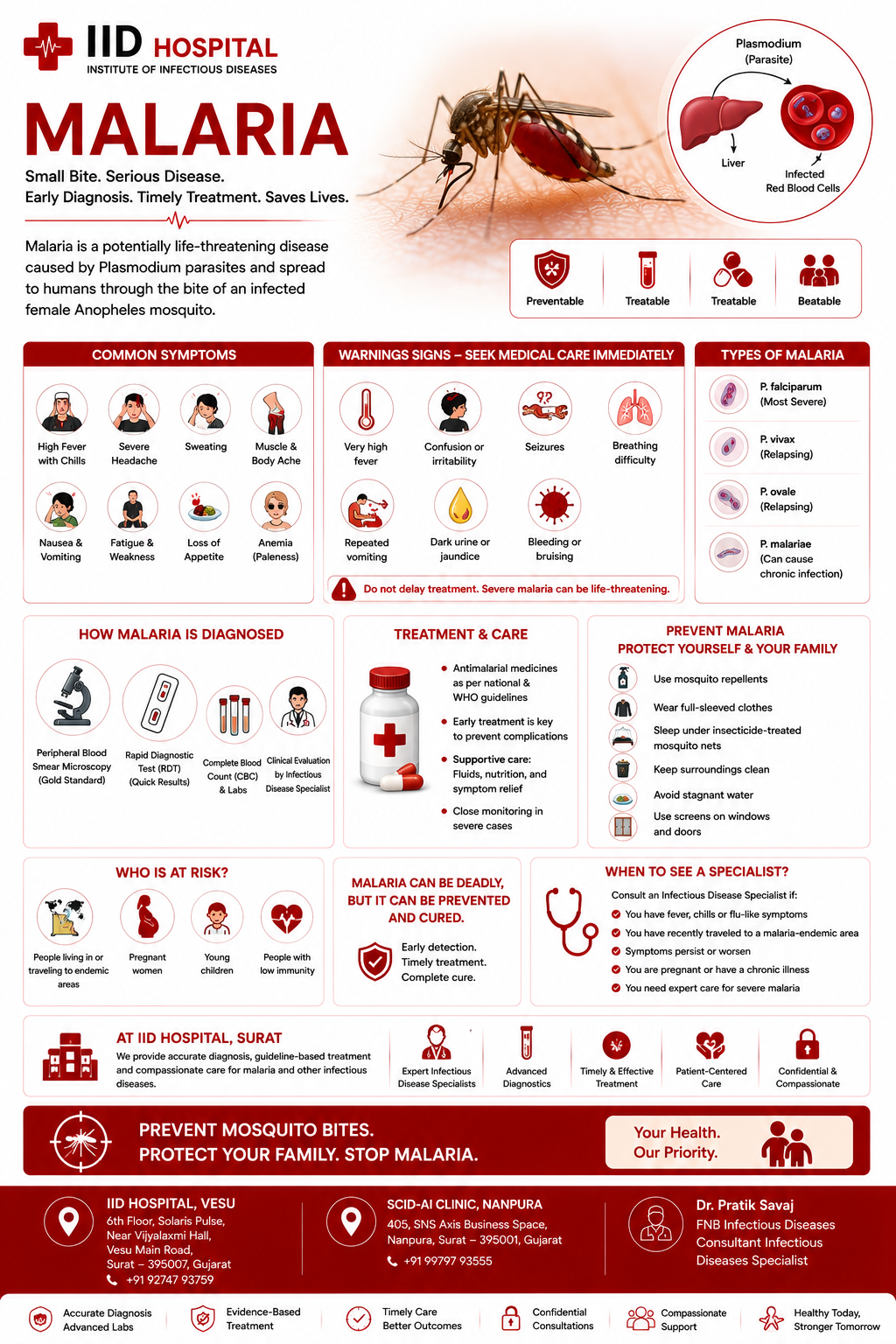
Malaria
Four Plasmodium species cause malaria in Surat — falciparum (most dangerous) and vivax (most common). Species identification is non-negotiable: falciparum requires combination ACT; vivax requires primaquine radical cure to prevent relapse from liver dormant forms.
Symptoms
IID Hospital Protocol
Typhoid Fever
The Widal test should never guide typhoid treatment in Surat — it is unreliable in an endemic city. Blood culture with antibiotic sensitivity testing is the correct approach. Fluoroquinolone-resistant and XDR typhoid are increasingly common in Surat — empirical ciprofloxacin will fail in many cases.
Symptoms
IID Hospital Protocol
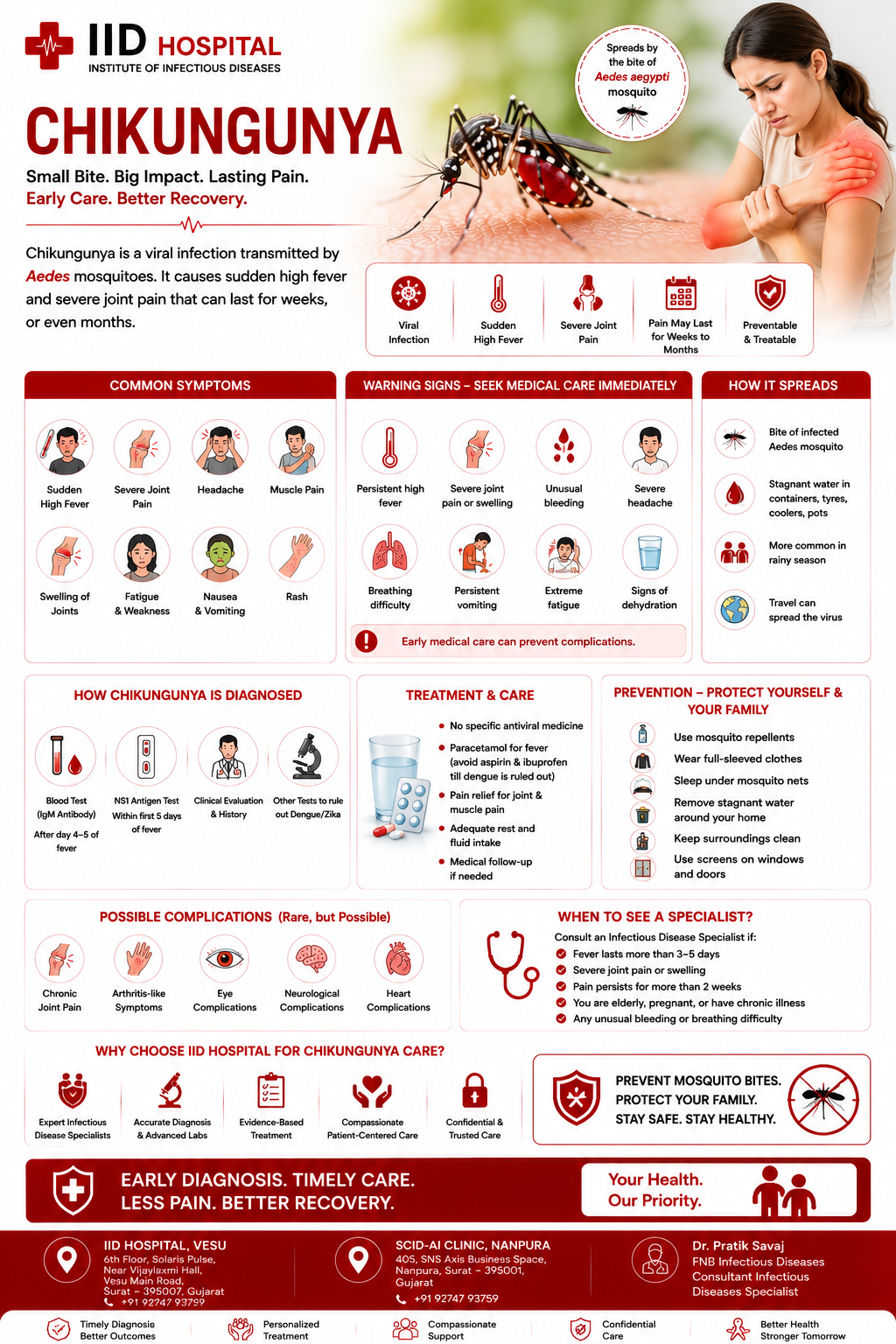
Chikungunya
The fever resolves in 2–4 days. The joint pain may last months. Post-chikungunya arthritis (PCA) affects 30–40% of patients — bilateral, symmetrical, immune-mediated joint inflammation that requires hydroxychloroquine and physiotherapy, not just paracetamol and waiting. Always test for dengue simultaneously.
Symptoms
IID Hospital Protocol
Leptospirosis & Scrub Typhus
Two commonly missed fever diagnoses in Surat. Leptospirosis peaks after monsoon flooding — fever + jaundice + muscle pain after water exposure. Scrub typhus presents with an eschar (painless black ulcer at mite bite site) that is frequently overlooked. Both respond dramatically to doxycycline — making doxycycline both treatment and a diagnostic test.
Leptospirosis
Scrub Typhus

A vaccine-preventable viral haemorrhagic fever transmitted by the Aedes mosquito. Mandatory vaccination for travel to Africa and South America. Yellow fever does not occur in India but returning travellers can present with it — and IID Hospital provides the Yellow Fever vaccination certificate required for international travel.
Symptoms
Prevention & Treatment
Travel Advisory
Travelling to Africa or South America? Yellow Fever vaccination is legally mandatory — immigration at your destination will require the International Certificate of Vaccination (yellow card). Book your vaccination at IID Hospital at least 10 days before departure.

Surat’s Monsoon — When Every Fever Needs Expert Assessment
Surat’s monsoon season is medically unique — multiple infectious agents circulate simultaneously, all presenting with fever, making accurate diagnosis a genuine clinical challenge. The Aedes mosquito (dengue and chikungunya), the Anopheles mosquito (malaria), Salmonella typhi (typhoid from contaminated water), and Orientia tsutsugamushi (scrub typhus from mite bites) all peak between July and November.
In this environment, the same fever on day 1 could be any of six different conditions. Each requires a different test on a different schedule, a different treatment, different monitoring, and carries different risks if missed or mismanaged. This is the clinical reality that makes specialist assessment valuable for any persistent fever during Surat monsoon.
July — August
Peak Viral & Early Dengue
Schools reopen, indoor crowding, high humidity. Respiratory viral illnesses surge. Dengue cases begin rising as Aedes mosquito populations build after first rains. NS1 testing on day 1 for all fever.
August — September
Peak Dengue & Malaria
Mosquito populations peak. Dengue and malaria at highest levels. Chikungunya also active. Every fever requires NS1 + blood smear on day 1. Critical phase dengue needs daily platelet monitoring.
September — October
Typhoid & Leptospirosis Season
Monsoon flooding contaminates water supplies. Typhoid cases peak. Leptospirosis from flood water exposure. Blood culture before antibiotics is non-negotiable. XDR typhoid emerging in Surat.
October — November
Post-Monsoon Persistence
Dengue and malaria decline slowly. Vivax malaria relapses appear. Scrub typhus cases in green areas around Surat. Post-chikungunya arthritis presenting in patients infected 2–3 months earlier.
The Monsoon Protocol at IID Hospital
For any fever July–November in Surat: NS1 antigen + blood smear + RDT + CBC on day 1. Paracetamol only — no NSAIDs until dengue excluded. Blood culture if fever persists beyond day 5 or typhoid is suspected. Repeat smear if first malaria smear is negative but clinical suspicion remains high.

When Fever Has No Answer — The FUO Workup
Fever of Unknown Origin (FUO) is classically defined as fever above 38.3°C persisting for more than 3 weeks with no diagnosis despite initial basic investigation. In practice at IID Hospital, Dr. Savaj investigates any fever lasting beyond 2–3 weeks without a clear cause. FUO is not a diagnosis — it is a prompt to investigate systematically rather than treat empirically.
The three broad categories of FUO — infectious, malignant, and inflammatory — require completely different investigation pathways. Randomly ordering tests is inefficient; a structured sequential protocol that matches investigation to clinical probability is the specialist approach. In India, tuberculosis is the most common cause of FUO — and is frequently overlooked because it can affect any organ with a normal chest X-ray.
Book FUO AssessmentInfectious Causes — Most Common
Tuberculosis (most common in India — any organ); infective endocarditis; liver abscess; intra-abdominal abscess; HIV; brucellosis; typhoid with atypical presentation; Q fever; visceral leishmaniasis.
Malignant Causes
Lymphoma (most common malignant FUO cause); leukaemia; renal cell carcinoma; hepatocellular carcinoma; colon cancer with occult fever; other solid organ malignancies with systemic inflammation.
Inflammatory & Autoimmune Causes
Adult-onset Still’s disease (AOSD); systemic lupus erythematosus (SLE); vasculitis (temporal arteritis, PAN); inflammatory bowel disease; sarcoidosis; drug fever; thyroiditis.
Undiagnosed Despite Full Workup
A proportion of FUO cases remain undiagnosed after comprehensive investigation. Many resolve spontaneously. In these cases, watchful waiting and periodic reassessment is preferable to empirical treatment.
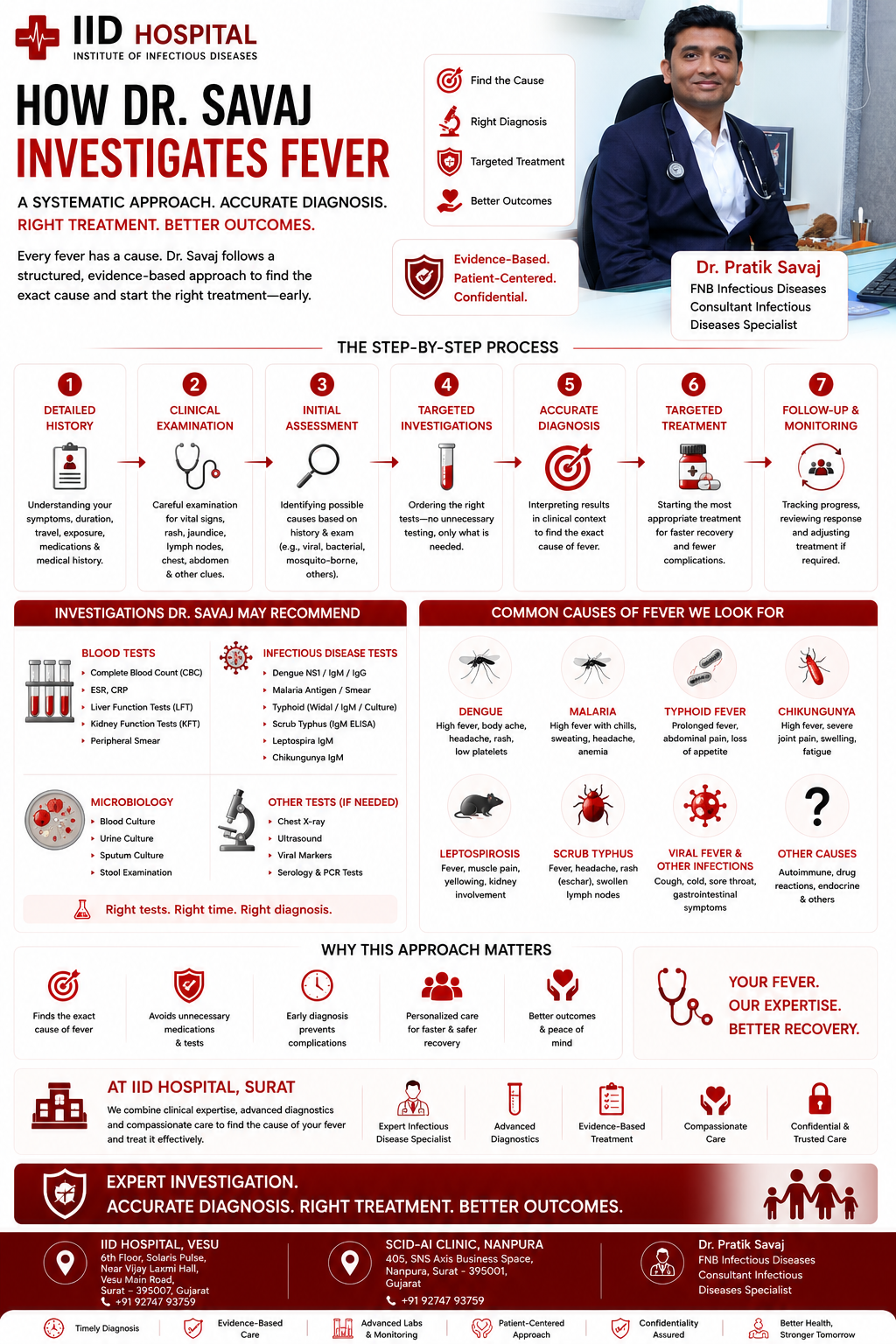
How Dr. Savaj Investigates Fever — Step by Step
Complete History — The Most Important Step
Before any testTravel history, occupational exposure, water and food sources, animal contact, sexual history, medication history, prior infections, and complete symptom timeline. In infectious disease, a thorough history narrows the differential more than any single test. Knowing that the patient was near flood water (leptospirosis), works in scrub vegetation (scrub typhus), or had a recent unprotected exposure (HIV) changes the entire investigation pathway.
Day 1–3 Tests — Catch What’s Most Dangerous First
Monsoon fever priorityNS1 antigen (dengue — most sensitive days 1–5); Blood smear + RDT (malaria — all species); CBC with platelets (falling platelets = dengue; severe anaemia = malaria); LFT (elevated transaminases in dengue and leptospirosis). These four tests exclude the two most dangerous and common monsoon fevers on day 1.
Day 5+ Tests — If Fever Persists
After 5 days of feverBlood culture before any antibiotic (typhoid — gold standard); Dengue IgM (now detectable); Chikungunya IgM; Typhidot IgM; Weil-Felix / Leptospira IgM (leptospirosis); Scrub typhus IgM (if eschar or unexplained fever in someone with outdoor exposure). Serology tests become reliable only after day 5 — sending them earlier produces false negatives.
Extended FUO Workup — Fever Beyond 2–3 Weeks
If fever persistsTB workup: GeneXpert sputum, IGRA, CXR, CT chest and abdomen; Infective endocarditis: echocardiogram + blood cultures x3; Malignancy screen: LDH, uric acid, PET-CT or CT-guided biopsy; Autoimmune: ANA, anti-dsDNA, ANCA, RF, ferritin (AOSD); HIV test — mandatory in all FUO workups. The sequence follows clinical probability — the most likely cause in the local context is investigated first.
Culture-Guided Treatment — Never Empirical Antibiotics for Fever
After diagnosisEmpirical antibiotics for undifferentiated fever mask the diagnosis, reduce culture yield, and drive resistance. Treatment at IID Hospital follows diagnosis. Where urgency demands empirical treatment (malaria with deterioration, severe typhoid), the most targeted appropriate drug is used based on local resistance patterns — not the broadest available antibiotic. Every typhoid case has blood culture + AST before the first antibiotic where possible.
What to Bring to Your Appointment
Manage at Home (Symptomatically)
What to Do at Home
Paracetamol only (not ibuprofen during monsoon). 3–4 litres of fluids daily. Rest. Monitor temperature twice daily. If not improving by day 5, see Dr. Savaj.
See Dr. Savaj Urgently
Call Immediately
+91 92747 93759 — Dr. Pratik Savaj, IID Hospital, Surat. Mon–Sat 11AM–1PM & 4–6PM. For urgent concerns outside clinic hours — WhatsApp.
What Patients Say About Dr. Pratik Savaj
I had fever for 3 weeks and was told it was viral fever by 3 different doctors. Dr. Savaj did a systematic workup and found extrapulmonary TB in a lymph node biopsy on day 3. My chest X-ray was perfectly normal. He knew exactly what to look for and in what order.
During dengue, Dr. Savaj monitored my platelet count every day and told me exactly when I needed to worry. My platelets fell to 28,000 but he managed it without hospitalisation. His calm, clear communication made a frightening week manageable.
My typhoid was treated with ciprofloxacin for 10 days at another clinic — no improvement. Dr. Savaj sent a blood culture on day 1, found fluoroquinolone-resistant typhoid, and switched to the right antibiotic. I recovered in 5 days. No one had tested for resistance before.
I had dengue with a platelet count below 30,000. Dr. Savaj monitored me daily, explained every number, and told me exactly when to worry and when not to. I avoided unnecessary hospitalisation and recovered fully at home.
Three weeks of fever, multiple negative tests elsewhere. Dr. Savaj ran the right panel, confirmed typhoid, and started targeted treatment. Fever broke within 48 hours. I wish I had come here first.
Fever for 6 weeks with no diagnosis. Dr. Savaj worked through a systematic FUO protocol, found the cause no one else had looked for, and treated it correctly. The most thorough doctor I have seen.
Questions Patients Ask
Before Their First Appointment
Answered by Dr. Pratik Savaj, FNB Infectious Diseases — IID Hospital, Vesu, Surat.