
Expert Tuberculosis Care in Surat
By Dr. Pratik Savaj — FNB Infectious Diseases
IID Hospital provides complete TB care — GeneXpert diagnosis, DOTS supervision, drug-sensitive and drug-resistant TB management, HIV-TB co-infection, extrapulmonary TB, and isoniazid preventive therapy. Dr. Pratik Savaj, FNB Infectious Diseases, has specific training in complex TB from P.D. Hinduja Hospital, Mumbai.
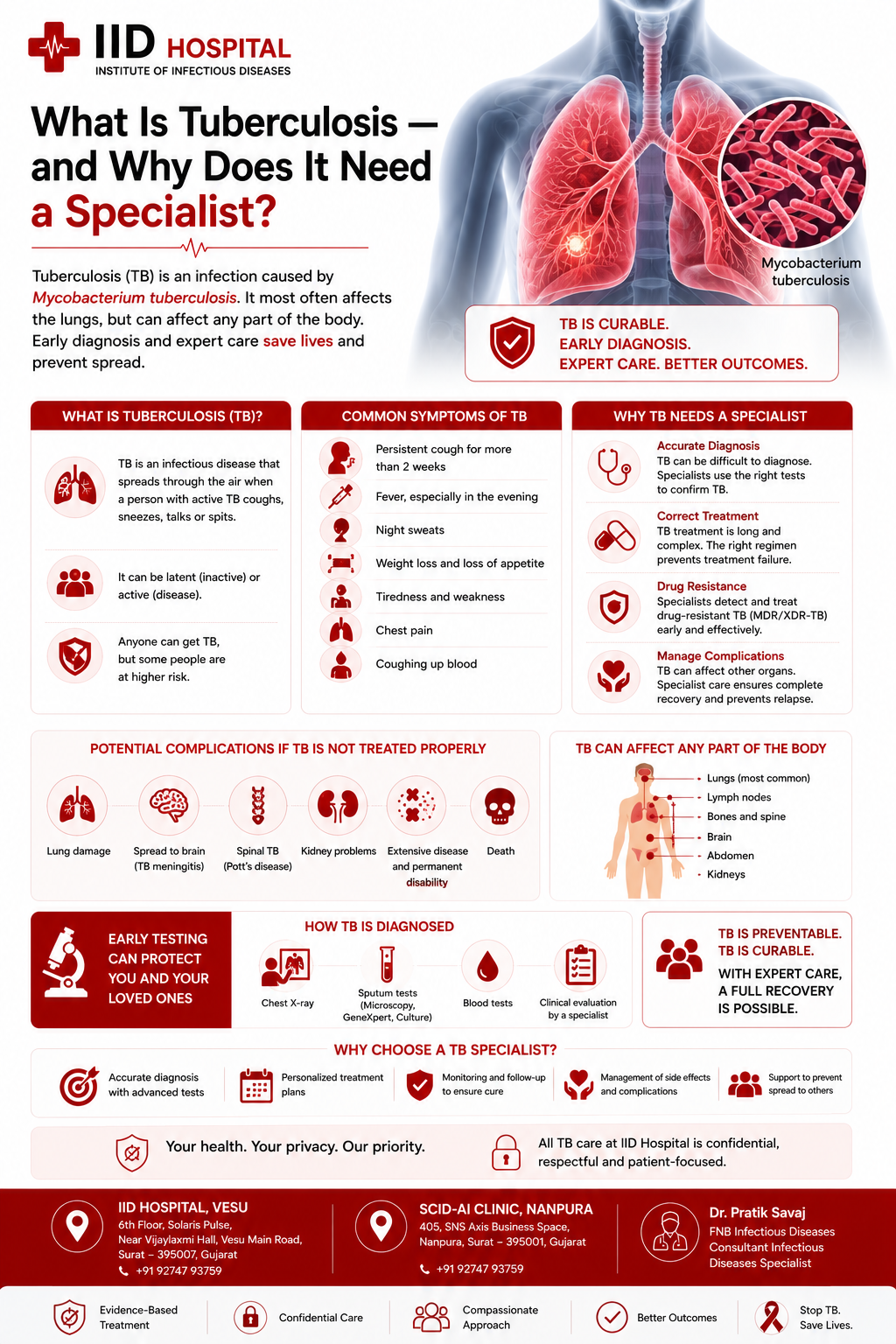
What Is Tuberculosis — and Why Does It Need a Specialist?
Tuberculosis is caused by Mycobacterium tuberculosis — a slow-growing bacterium that primarily infects the lungs but can affect virtually any organ. It spreads through the air when a person with active pulmonary TB coughs, sneezes, or speaks — releasing microscopic droplet nuclei that can remain suspended in the air for hours.
TB is uniquely complex for three reasons. First, it is slow — the bacterium divides every 20–24 hours (most bacteria divide in 20–30 minutes), which is why treatment takes months, not days. Second, it hides — latent TB infection allows the bacterium to persist dormant in the body for decades before reactivating. Third, it develops drug resistance when treatment is inadequate, creating strains that are far harder and more expensive to treat.
India has the world’s highest TB burden — 2.8 million new cases per year. TB is curable with the right diagnosis, the right drugs, and completion of the full course. Specialist care matters most when standard approaches have failed, when drug resistance is present, or when TB affects organs outside the lungs.
Why TB Needs a Specialist
Key TB Facts
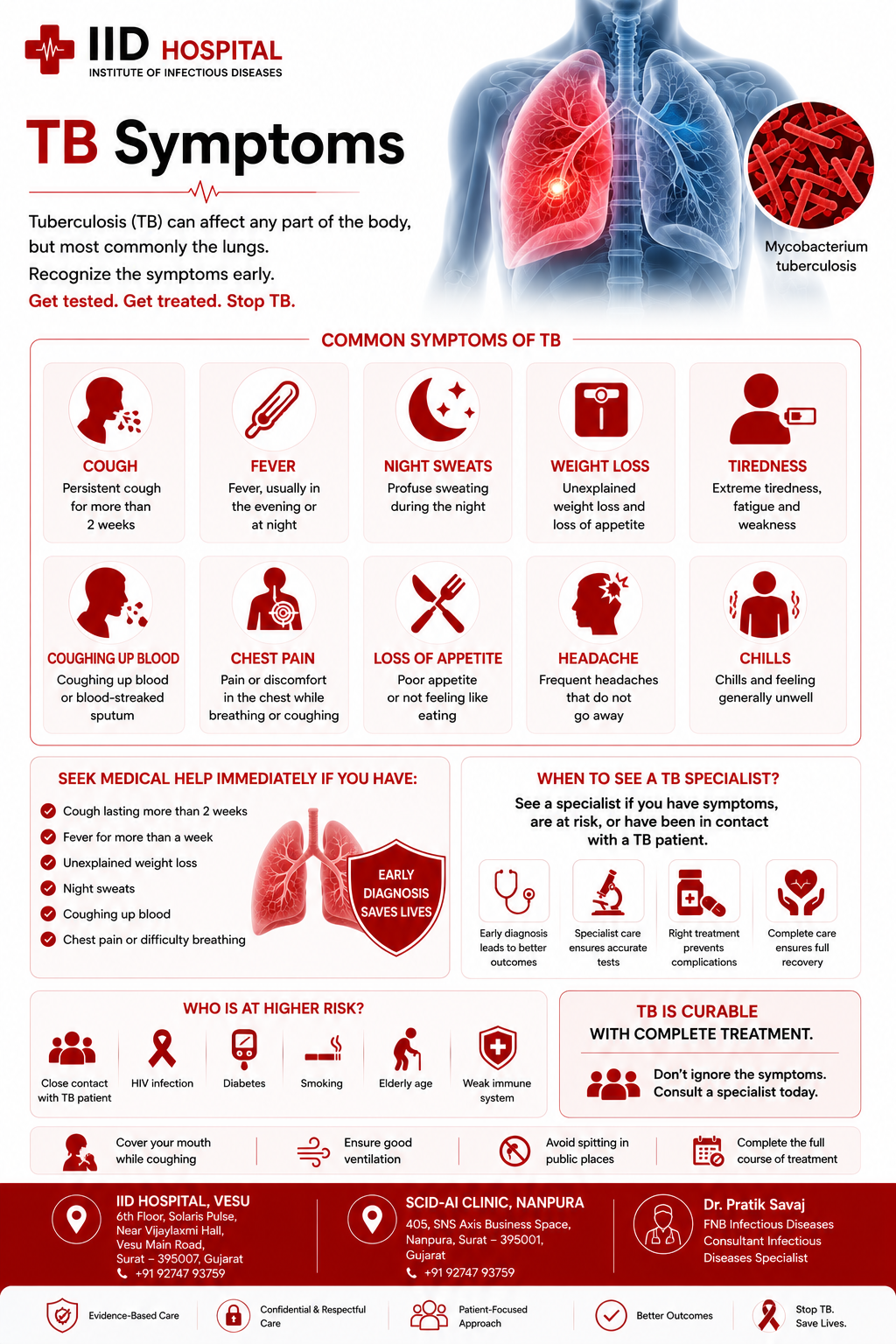
TB Symptoms — When to See a Specialist
TB symptoms develop slowly over weeks to months — not suddenly like dengue or malaria. This gradual onset is one reason TB is frequently diagnosed late. The constitutional symptoms (fever, night sweats, weight loss) occur in both pulmonary and extrapulmonary forms.
Extrapulmonary TB — No Cough, Normal Chest X-Ray
See Dr. Savaj If
Cough lasting more than 2 weeks; unexplained weight loss with fever; any persistent swollen lymph nodes; fever of unknown origin; back pain with neurological signs; or any fever in an HIV-positive patient. In Surat’s endemic setting, TB must be actively excluded — not passively assumed absent.
High-Risk Groups in Surat
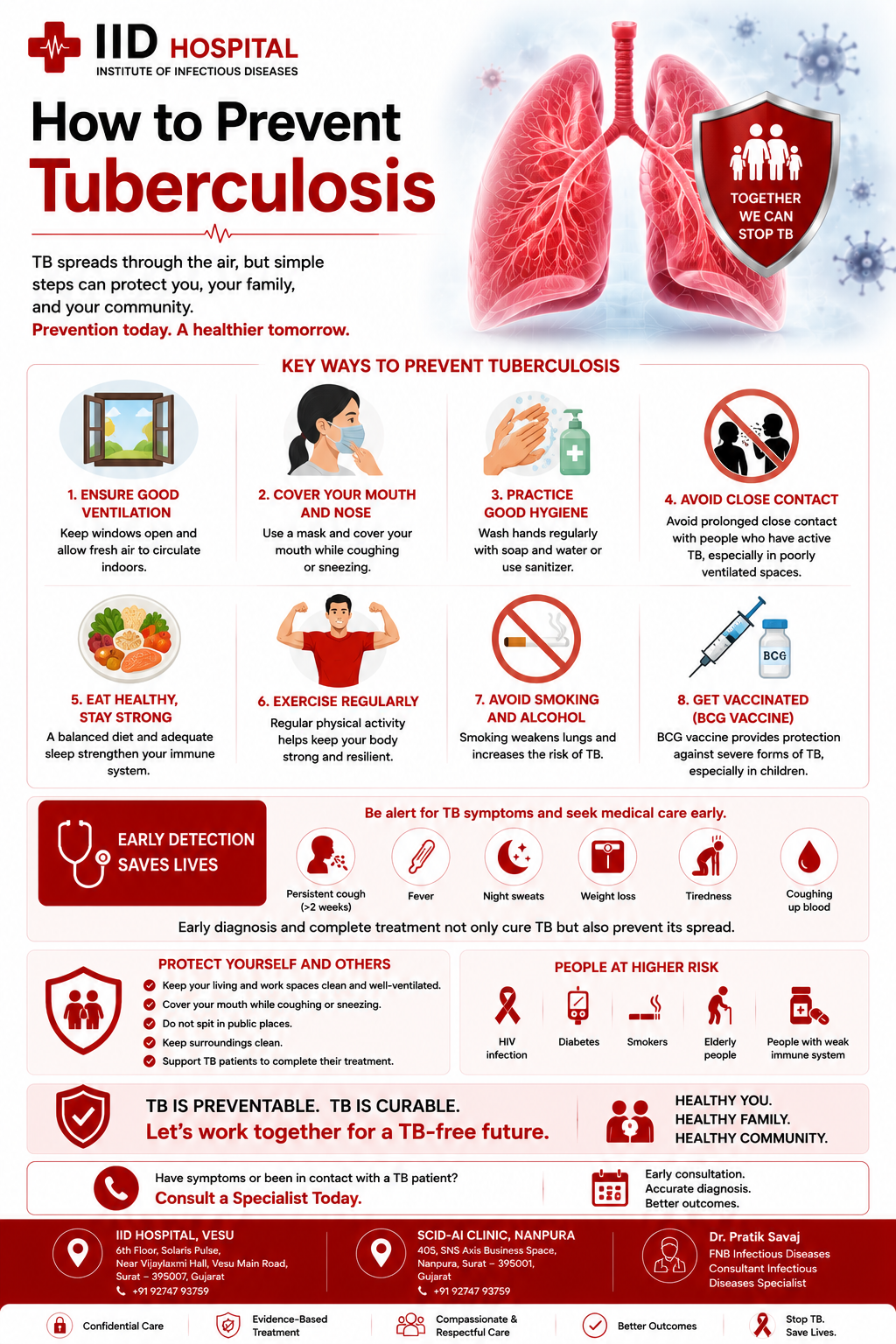
How to Prevent Tuberculosis
TB prevention operates at three levels: preventing exposure, preventing progression from latent to active TB, and preventing transmission from active cases to contacts. Each level has specific evidence-based interventions.
BCG Vaccination at Birth
BCG is given to all newborns under India’s Universal Immunisation Programme. It provides strong protection against severe childhood TB forms — TB meningitis and miliary TB. All children should receive BCG within 24 hours of birth.
Isoniazid Preventive Therapy (IPT)
6 months of daily isoniazid for high-risk contacts with latent TB. Recommended for: all HIV-positive patients (after excluding active TB), children under 5 who are household contacts, and immunocompromised individuals with positive IGRA/TST. Reduces reactivation risk by 60–90%.
Respiratory Precautions for Active TB Patients
Patients with active pulmonary TB should wear a surgical mask around others until sputum converts negative on treatment; ensure adequate natural ventilation; avoid crowded enclosed spaces; and not share sleeping spaces with children or immunocompromised people during the infectious period.
Contact Investigation and Screening
Every household contact of a TB patient should be evaluated — not just symptomatic ones. Children under 5 and immunocompromised contacts are priority. IGRA/TST identifies latent TB. GeneXpert and CXR exclude active TB. IID Hospital includes all household members in contact assessment.
ART for HIV-Positive Individuals
HIV-positive individuals are 20 times more likely to develop active TB. ART reduces TB risk by 60–65% by restoring immune function. Combined ART + IPT is the most powerful TB prevention strategy for HIV-positive individuals.
Complete TB Treatment — Prevent Drug Resistance
Every patient who starts TB treatment must complete the full course. Stopping early allows surviving bacteria to develop resistance and infect others. Completing TB treatment is an act of community prevention, not just personal treatment.
Free TB Prevention in India
India’s NTEP provides: free BCG for all newborns; free isoniazid for preventive therapy; free IGRA testing at designated centres; and free contact investigation for household contacts. Dr. Savaj coordinates with NTEP for eligible patients.
Forms of Tuberculosis Treated at IID Hospital
TB is not a single condition — it is a family of diseases caused by Mycobacterium tuberculosis affecting different organs, with different presentations, different diagnostic approaches, and in the case of drug-resistant forms, completely different treatment regimens.
TB Can Occur Without a Cough
Extrapulmonary TB — TB affecting lymph nodes, spine, abdomen, brain, kidneys — presents with no respiratory symptoms and a normal chest X-ray. This is why many extrapulmonary TB cases are diagnosed late. At IID Hospital, TB is actively considered in any patient with persistent unexplained fever, swollen glands, or organ-specific symptoms — regardless of chest findings.
Pulmonary TB
Lung involvement — most common form
Extrapulmonary TB
Lymph node, spine, brain, abdomen
Latent TB Infection
Infected but not ill — no symptoms
MDR-TB
Resistant to isoniazid + rifampicin
Pre-XDR & XDR-TB
Additional resistance — most complex
HIV-TB Co-Infection
Requires integrated specialist management
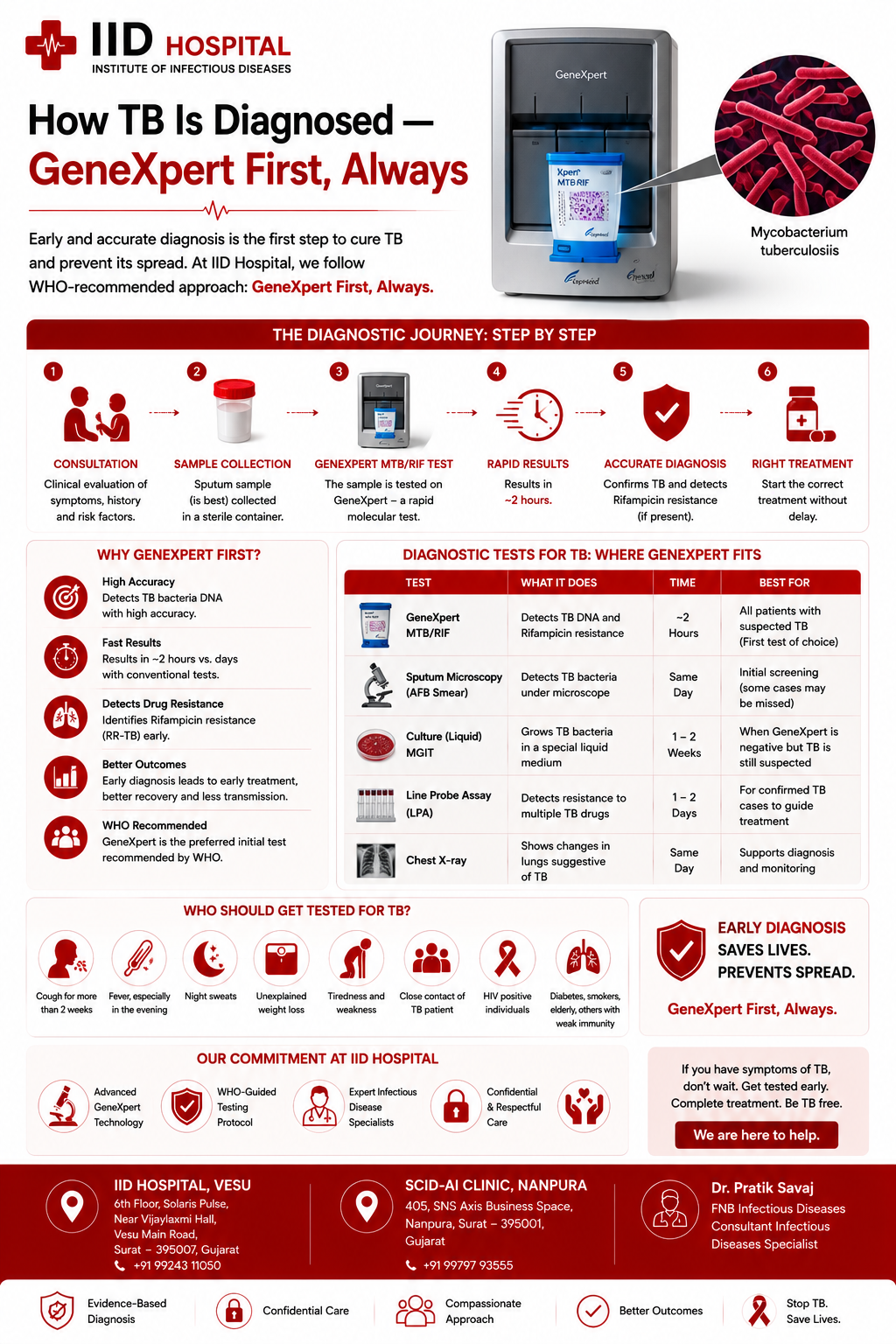
How TB Is Diagnosed — GeneXpert First, Always
GeneXpert MTB/RIF — First-Line Test
Always before starting treatmentGeneXpert simultaneously detects Mycobacterium tuberculosis and rifampicin resistance in 2 hours from a single sputum sample. Sensitivity 85–90% — far higher than sputum smear (50–60%). Rifampicin resistance on GeneXpert = highly predictive of MDR-TB, requiring immediate management change. At IID Hospital, GeneXpert is not an add-on after smear negativity — it is the first-line diagnostic for all suspected TB cases.
Sputum Culture + Drug Sensitivity Testing (DST)
Gold standard — 4–8 weeksMGIT liquid culture (4–8 weeks) grows the organism and allows comprehensive drug sensitivity testing against all first and second-line drugs. Essential for: confirming MDR-TB suspected on GeneXpert; guiding second-line regimen selection for MDR/XDR-TB; and resolving discordant GeneXpert results. Culture also confirms diagnosis when GeneXpert is negative in strong clinical suspicion.
Chest X-Ray + HRCT Thorax
Anatomical extent of diseaseChest X-ray provides immediate visual assessment of lung involvement. HRCT (high-resolution CT) thorax gives more detail — cavities, nodules, tree-in-bud pattern — useful in sputum-negative cases, assessing extent of disease, and monitoring treatment response. Important: a normal chest X-ray does not rule out TB — extrapulmonary TB has no lung findings.
IGRA / Tuberculin Skin Test (TST)
Latent TB diagnosisInterferon-gamma release assay (IGRA) — a blood test — or TST detects immune sensitisation to TB antigens, indicating latent TB infection. Used for: contact investigation of TB cases, screening of HIV patients for preventive therapy, and assessing immunocompromised patients before immunosuppressive drugs. IGRA is more specific than TST in BCG-vaccinated individuals (which is virtually everyone in India).
Biopsy + Histopathology (Extrapulmonary TB)
Essential for extrapulmonary formsFor lymph node, pleural, pericardial, abdominal, or tissue TB — tissue biopsy with GeneXpert on the specimen and histopathology showing caseating granulomas is the diagnostic approach. Fine needle aspiration cytology (FNAC) of enlarged lymph nodes, guided by ultrasound, provides tissue without open surgery. This is often the only way to diagnose extrapulmonary TB that has been missed by chest-focused investigations.
HIV Test — Mandatory in All TB Patients
Non-negotiable at IID HospitalEvery TB patient at IID Hospital is offered and recommended HIV testing. HIV status fundamentally changes TB management: ART timing, drug selection, IRIS risk, IPT for contacts. Missing HIV in a TB patient means managing TB without the most important prognostic co-factor. Fully confidential under HIV Act 2017.
Don’t Start Antibiotics Before Testing
A single dose of rifampicin or fluoroquinolones can sterilise a sputum sample and produce a false-negative GeneXpert. Always collect sputum for GeneXpert before starting any antibiotic — including broad-spectrum drugs like levofloxacin, moxifloxacin, or azithromycin.
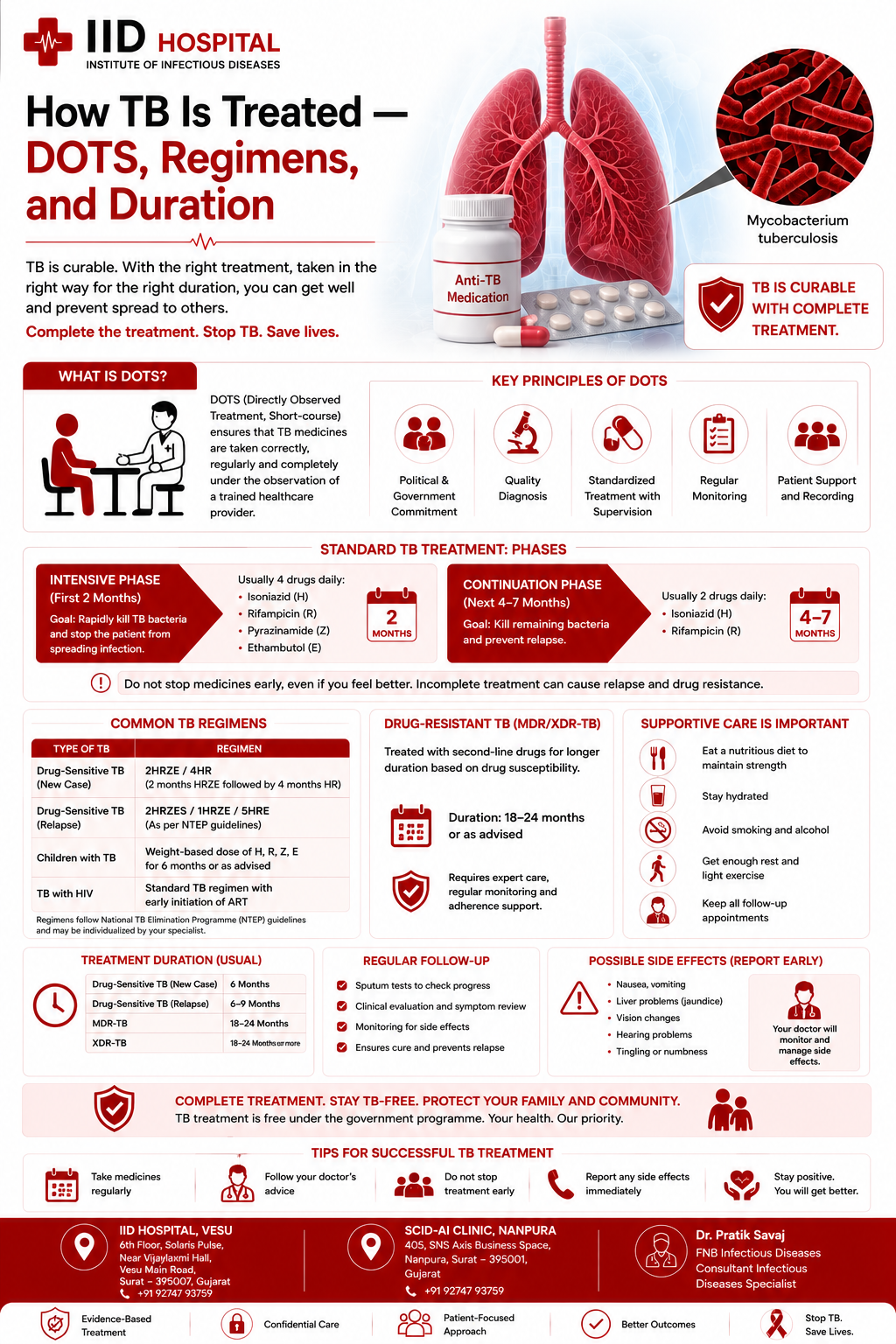
How TB Is Treated — DOTS, Regimens, and Duration
TB treatment is antibiotic therapy — but the specifics matter enormously. The right drugs, the right doses, for the full duration, under DOTS supervision (to ensure every dose is taken) are the pillars of treatment success. Inadequate treatment drives drug resistance.
DOTS — Why Every Dose Must Be Supervised
Directly Observed Treatment Short-course (DOTS) means a trained healthcare worker watches the patient swallow every dose. This is not punitive — it is the evidence-based standard that prevents drug resistance. When patients take TB drugs inconsistently or stop early, surviving bacteria develop resistance. DOTS eliminates this risk. At IID Hospital, Dr. Savaj supervises DOTS or coordinates with NTEP DOTS centres for all TB patients.
MDR-TB & XDR-TB
When Standard Treatment Fails
Drug-resistant TB is India’s most urgent TB crisis. India has the world’s largest MDR-TB burden — over 130,000 new cases per year. MDR-TB develops when drug-sensitive TB is treated with wrong drugs, wrong doses, interrupted treatment, or poor-quality medications. Once drug resistance develops, treatment becomes vastly more complex, more toxic, more prolonged, and less successful.
At IID Hospital, Dr. Savaj has specific training in MDR-TB management from his fellowship at P.D. Hinduja Hospital — one of India’s principal MDR-TB centres. He manages culture-confirmed MDR-TB with individualised regimens based on DST, coordinates free NTEP second-line drugs, and provides monthly monitoring of treatment response and drug toxicity.
Book MDR-TB Consultation| Resistance Type | Drugs Resistant To | Treatment | Success Rate |
|---|---|---|---|
| Drug-Sensitive (DS-TB) | Sensitive to all | HRZE × 2 + HR × 4 | 95%+ |
| Isoniazid-Resistant (Hr-TB) | Isoniazid only | RZE + fluoroquinolone × 6m | 85–90% |
| MDR-TB | Isoniazid + Rifampicin | BPaLM or BDQ-based × 18–24m | 55–65% |
| Pre-XDR-TB | MDR + Fluoroquinolone | Individualised × 20–24m | 40–55% |
| XDR-TB | Pre-XDR + BDQ or LZD | Individualised specialist team | <40% — specialist centre |
Warning Signs of MDR-TB
Complete TB Care — All Under One Roof
GeneXpert-First Diagnosis
GeneXpert MTB/RIF as the first-line test for all suspected TB — not an add-on after smear negativity. Same-day rifampicin resistance detection. Sputum culture + full DST for all cases. Extrapulmonary biopsy coordination.
DOTS Supervision
Directly Observed Treatment for all drug-sensitive TB. Dr. Savaj is a private DOTS provider or coordinates with NTEP DOTS centres. Monthly sputum monitoring during treatment. Free NTEP drugs coordinated for eligible patients.
MDR-TB & XDR-TB Management
Specific training from P.D. Hinduja Hospital. Culture-confirmed MDR-TB managed with DST-guided second-line regimens including bedaquiline-based BPaLM. Monthly culture monitoring, cardiac QTc monitoring, drug toxicity management.
HIV-TB Co-Infection
Integrated HIV-TB management: ART timing (2 weeks if CD4 <50), drug interaction management (rifampicin+dolutegravir/efavirenz), IRIS recognition and management, and isoniazid preventive therapy for HIV contacts.
Contact Investigation & IPT
Household contact evaluation, IGRA/TST for latent TB detection. Isoniazid preventive therapy (6 months) for contacts with latent TB — especially children under 5 and immunocompromised household members. Reduces reactivation risk by 60–90%.
Extrapulmonary TB Diagnosis
Lymph node, spinal, meningeal, abdominal, pleural, and renal TB. Tissue biopsy coordination, GeneXpert on biopsy specimens, CSF analysis for TB meningitis, and prolonged 9–12 month treatment protocols.

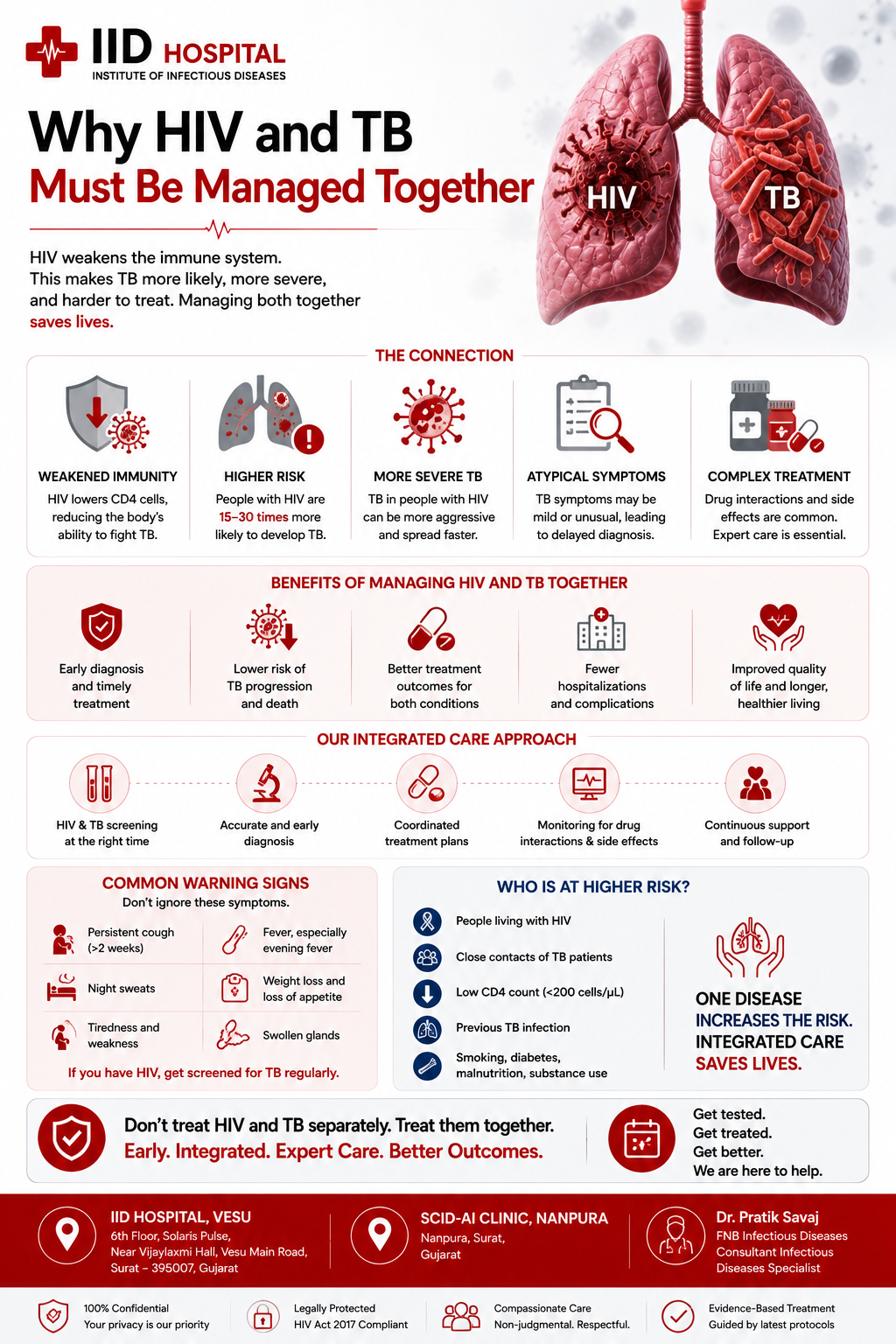
Why TB and HIV Must Be Managed Together
HIV suppresses the CD4 T-cells that contain latent TB. This makes HIV-positive individuals 20 times more likely to develop active TB. TB in turn accelerates HIV by triggering immune activation and increasing viral replication. Managing one without the other produces consistently inferior outcomes.
Every TB Patient at IID Hospital Is Offered HIV Testing
This is a non-negotiable clinical standard at IID Hospital — not optional. HIV status changes every aspect of TB management: ART timing, drug selection, monitoring, IPT for contacts, and prognosis. All HIV testing is fully confidential under HIV Act 2017.
What Patients Say About Dr. Pratik Savaj
I had fever for 3 weeks, cough for 6 weeks, and a normal chest X-ray. Four doctors treated me for viral fever and sinusitis. Dr. Savaj did GeneXpert on my sputum on day 1 — positive for TB. He then found lymph node involvement with biopsy. I had extrapulmonary TB that had been completely missed.
My TB was not responding to the standard DOTS treatment. Dr. Savaj sent a sputum culture and DST. Found rifampicin resistance — MDR-TB. He changed my treatment to a bedaquiline-based regimen. Six months later, my sputum culture converted to negative. He literally saved my life.
My wife had TB and Dr. Savaj tested me and both my children. I had latent TB (IGRA positive). He put me on isoniazid preventive therapy for 6 months. My younger child was under 5 — he said this was the most important person to treat. One year on, we are all well. Thorough and caring.
My company required a chest X-ray and they found old TB scarring. Dr. Savaj explained the difference between latent and active TB clearly, started preventive isoniazid, and I completed the course without a single active episode. His explanation removed months of anxiety.
My brother had TB and our whole family was worried. Dr. Savaj tested every household member, started preventive therapy for those who needed it, and explained exactly how TB spreads. The right information made everything less frightening.
I had drug-resistant TB after a failed first course elsewhere. Dr. Savaj designed a second-line regimen, monitored every side effect, and coordinated with the district DOTS centre. Two years later I am culture-negative and cured. The specialist difference was everything.
Questions Patients Ask
Before Their First Appointment
Answered by Dr. Pratik Savaj, FNB Infectious Diseases — IID Hospital, Vesu, Surat.