Tuberculosis (TB)Causes, Symptoms, Diagnosis & Treatment
Tuberculosis is caused by Mycobacterium tuberculosis — a bacterium that primarily attacks the lungs. Despite being preventable and fully curable, TB remains the world’s leading infectious disease killer. India accounts for 28% of all global TB cases. With early GeneXpert diagnosis and complete 6-month treatment, TB is 100% curable.
global TB burden
resistance in 2 hours
What Is Tuberculosis?
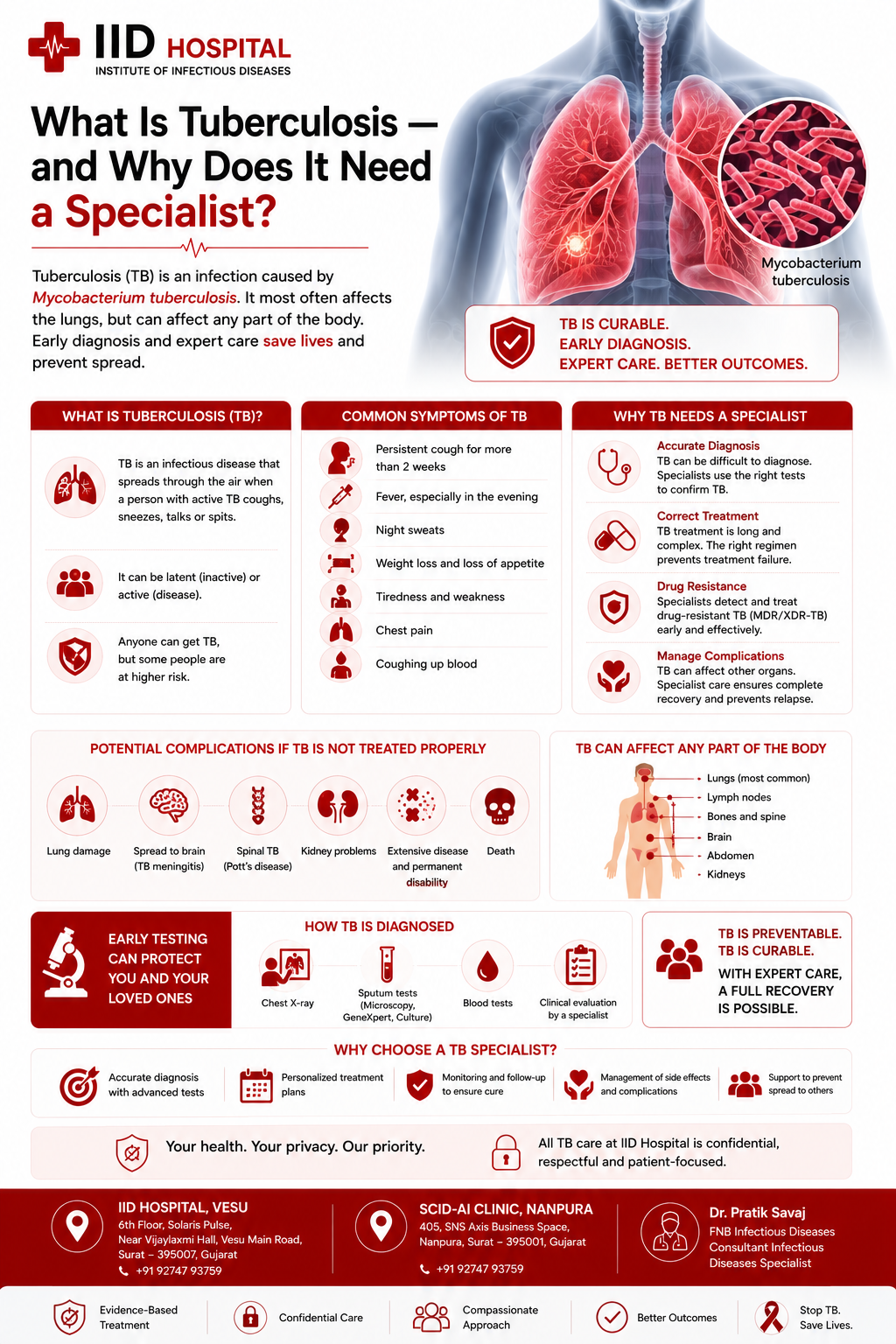
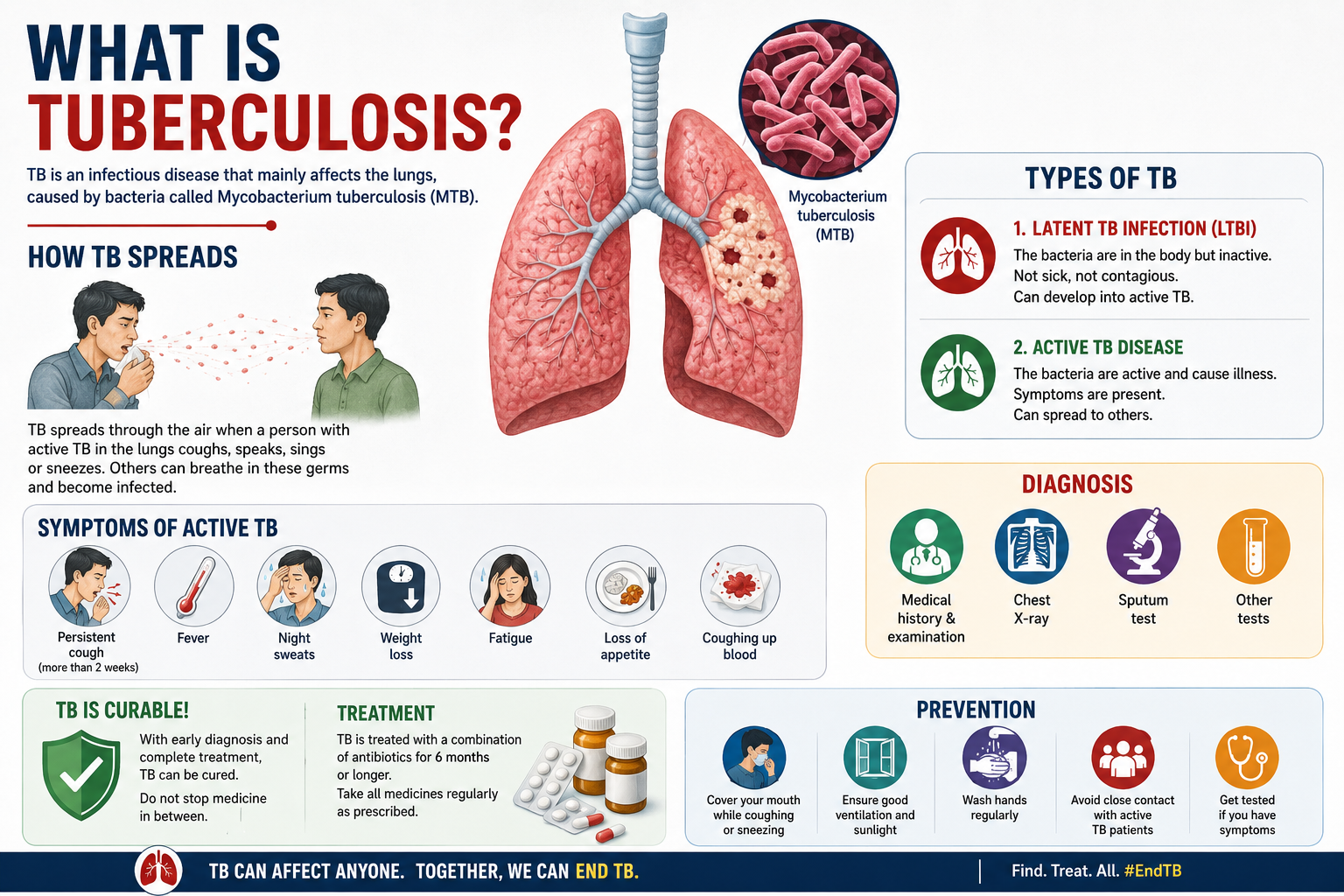
Tuberculosis is caused by Mycobacterium tuberculosis — a slow-growing, rod-shaped bacterium with a thick waxy cell wall made of mycolic acids. This wall makes it resistant to many antibiotics, allows it to survive inside immune cells, and is the reason TB treatment requires multiple drugs over several months.
M. tuberculosis has infected humans for thousands of years. Despite centuries of exposure, the human immune system has never fully eliminated it. Approximately one-quarter of the world’s population carries latent M. tuberculosis — contained by the immune system, not causing disease, but present and capable of reactivating.
Not everyone infected develops active TB. About 5–10% of people with latent TB infection (LTBI) will develop active TB in their lifetime — the risk is dramatically higher with HIV, diabetes, malnutrition, or immunosuppressant drugs.
Active TB
Latent TB (LTBI)
Normal Chest X-Ray Does Not Rule Out TB
Extrapulmonary TB can present with fever for weeks with a completely normal chest X-ray. TB lymphadenitis, abdominal TB, and miliary TB are all commonly missed because clinicians rely on a normal CXR to exclude TB. Always investigate with GeneXpert on relevant samples when clinical suspicion exists.

Dr. Pratik Savaj
FNB Infectious Diseases · IID Hospital, Surat
TB & HIV-TB co-infection specialist
TB Can Affect Any Organ
TB by Site — Clinical Presentation and Diagnosis
Each form of TB presents differently and requires specific diagnostic tests. Understanding the site of TB infection is essential — the same antibiotic regimen treats all forms, but the diagnostic path differs significantly.
Pulmonary TB (Lungs)
Presents with persistent cough 2+ weeks, blood in sputum, chest pain, night sweats, and weight loss. Infectious when active — droplet transmission. Diagnosed with sputum GeneXpert, smear, and chest X-ray. Standard 6-month HRZE/HR regimen is fully curative in drug-sensitive cases.
TB Lymphadenitis
Most common extrapulmonary TB. Painless swollen lymph nodes — typically cervical (neck). Chest X-ray is often completely normal, causing it to be dismissed as a gland infection. Diagnosis: lymph node FNAC or excision biopsy with GeneXpert. Most common in HIV-positive patients.
TB Meningitis
TB of the meninges (brain lining). Fever, headache, neck stiffness, confusion. High mortality without urgent treatment. Requires CSF GeneXpert, urgent CT head, immediate anti-TB drugs and corticosteroids. Most common in children and HIV-positive individuals.
Miliary TB
Haematogenous dissemination to multiple organs — lungs, liver, spleen, kidneys, brain. Classic CXR: diffuse tiny nodules throughout both lung fields. Requires aggressive anti-TB treatment. Most common in immunocompromised individuals.
Pott’s Disease (Spinal TB)
TB of the vertebrae — thoracic spine most common. Back pain, kyphosis, and in severe cases paraplegia from spinal cord compression. Requires MRI spine and urgent anti-TB treatment. Surgical decompression may be needed in neurological compromise.
Abdominal TB
TB of intestines, peritoneum, or abdominal lymph nodes. Abdominal pain, diarrhoea, ascites, and weight loss. Often confused with Crohn’s disease or malignancy. Diagnosis: colonoscopy biopsy, ascitic fluid GeneXpert, and CT abdomen. Very common in India.
Pulmonary TB (Lungs)
Presents with persistent cough 2+ weeks, blood in sputum, chest pain, night sweats, and weight loss. Infectious when active — droplet transmission. Diagnosed with sputum GeneXpert, smear, and chest X-ray. Standard 6-month HRZE/HR regimen is fully curative in drug-sensitive cases.
TB Lymphadenitis
Most common extrapulmonary TB. Painless swollen lymph nodes — typically cervical (neck). Chest X-ray is often completely normal, causing it to be dismissed as a gland infection. Diagnosis: lymph node FNAC or excision biopsy with GeneXpert. Most common in HIV-positive patients.
TB Meningitis
TB of the meninges (brain lining). Fever, headache, neck stiffness, confusion. High mortality without urgent treatment. Requires CSF GeneXpert, urgent CT head, immediate anti-TB drugs and corticosteroids. Most common in children and HIV-positive individuals.
Miliary TB
Haematogenous dissemination to multiple organs — lungs, liver, spleen, kidneys, brain. Classic CXR: diffuse tiny nodules throughout both lung fields. Requires aggressive anti-TB treatment. Most common in immunocompromised individuals.
Pott’s Disease (Spinal TB)
TB of the vertebrae — thoracic spine most common. Back pain, kyphosis, and in severe cases paraplegia from spinal cord compression. Requires MRI spine and urgent anti-TB treatment. Surgical decompression may be needed in neurological compromise.
Abdominal TB
TB of intestines, peritoneum, or abdominal lymph nodes. Abdominal pain, diarrhoea, ascites, and weight loss. Often confused with Crohn’s disease or malignancy. Diagnosis: colonoscopy biopsy, ascitic fluid GeneXpert, and CT abdomen. Very common in India.
Symptoms of Tuberculosis
TB symptoms depend on which organ is affected. Many patients have symptoms for weeks before seeking medical care — early recognition leads to earlier diagnosis and treatment.
The Red Flag Triad — Always Investigate for TB
The combination of prolonged fever + drenching night sweats + unexplained weight loss requires active TB investigation in India — even when the chest X-ray appears normal. GeneXpert on relevant samples and HRCT are needed to exclude extrapulmonary TB before dismissing these symptoms as non-specific.
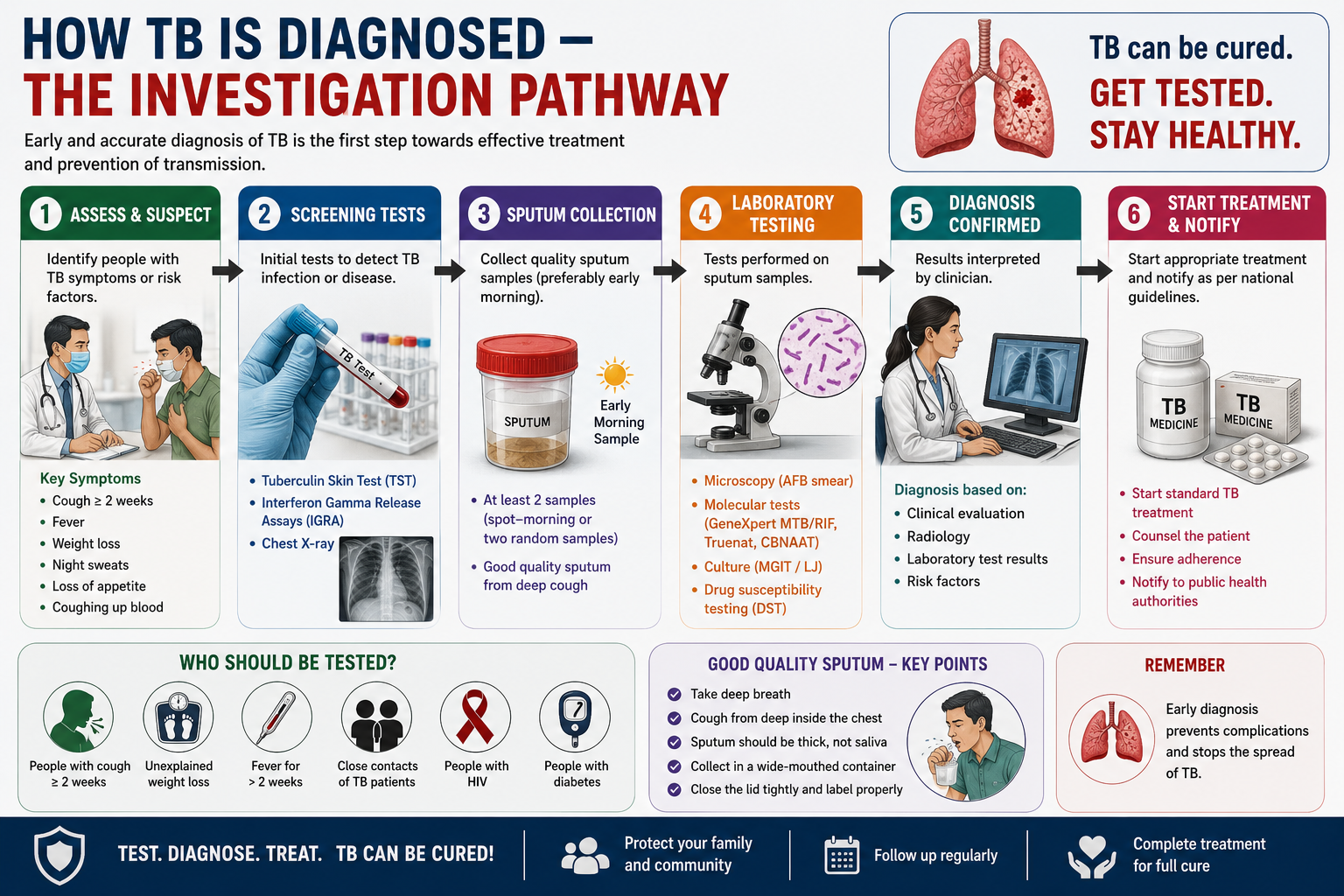
How TB Is Diagnosed — The Investigation Pathway
GeneXpert MTB/RIF (Xpert)
A molecular PCR-based test that detects M. tuberculosis DNA and identifies rifampicin resistance within 2 hours. Recommended as the first-line TB test by WHO and NTEP. Available free at all government DOTS centres. Can be used on sputum, lymph node aspirates, CSF, pleural fluid, urine, and tissue. Sensitivity approximately 88% — far superior to smear microscopy. A positive GeneXpert confirms TB and simultaneously indicates whether rifampicin resistance (a surrogate for MDR-TB) is present.
Sputum Smear Microscopy (AFB)
Direct microscopic detection of acid-fast bacilli in sputum (Ziehl-Neelsen or auramine-rhodamine stain). Rapid, inexpensive, and available everywhere — but sensitivity of only 50–60%, meaning it misses up to half of pulmonary TB cases. Does not detect drug resistance. Most useful for assessing infectiousness and monitoring treatment response. Never rely on smear alone to rule out TB.
Mycobacterial Culture & Drug Sensitivity Testing (DST)
Culture on liquid (MGIT) or solid (Löwenstein-Jensen) medium is the most sensitive and definitive test — and the only way to obtain comprehensive drug sensitivity testing (DST) for all first and second-line drugs. Takes 2–6 weeks. Essential before starting MDR-TB treatment and in all suspected treatment failure cases. Culture DST guides which specific drugs to use in resistant TB.
Chest X-Ray and HRCT
Chest X-ray is the standard first imaging investigation. Classic findings: upper lobe infiltrates, cavities, consolidation, hilar lymphadenopathy, pleural effusion. A normal CXR does not rule out TB — particularly for extrapulmonary forms or early pulmonary disease. HRCT chest is more sensitive and should be ordered when clinical suspicion is high but X-ray is unremarkable.
Tissue Biopsy and Histopathology
For extrapulmonary TB, a tissue sample from the affected organ is often the only way to confirm the diagnosis definitively. Lymph node FNAC or excision for TB lymphadenitis. Pleural biopsy for TB pleuritis. Bone biopsy for spinal TB. Colonoscopic biopsy for abdominal TB. The sample is sent for GeneXpert, culture, and histopathology — the presence of caseating granulomas with Langhans giant cells is the hallmark of TB.
IGRA (QuantiFERON) and Tuberculin Skin Test (TST)
IGRA and TST detect immune response to M. tuberculosis antigens. They indicate past infection (latent TB) but cannot diagnose active TB and cannot distinguish active from latent infection. Used for LTBI screening in household contacts of TB patients, HIV-positive individuals, and people starting immunosuppressant therapy. A positive IGRA/TST in a symptomatic person does not confirm active TB — it only confirms prior infection.
Why GeneXpert Changed TB
TB Treatment — DOTS, Drug Regimens & Duration
TB treatment is based on DOTS (Directly Observed Treatment, Short-course) — a healthcare worker observes every dose. All first-line drugs are free under NTEP in fixed-dose combination tablets. The full course must be completed — stopping early causes relapse and drug resistance.
Treatment Duration by TB Type
First-Line Drugs (HRZE) Free under NTEP
Key MDR-TB Drugs Free at DR-TB centres
Why Completing Every Dose Is Non-Negotiable
Patients often feel well after 2–3 months and stop treatment. Stopping early is dangerous. Surviving bacteria — which are more resistant — multiply and cause relapse with MDR-TB requiring 9–18 months of more toxic, more expensive treatment. Every single dose of TB medication matters. DOTS exists to prevent this.
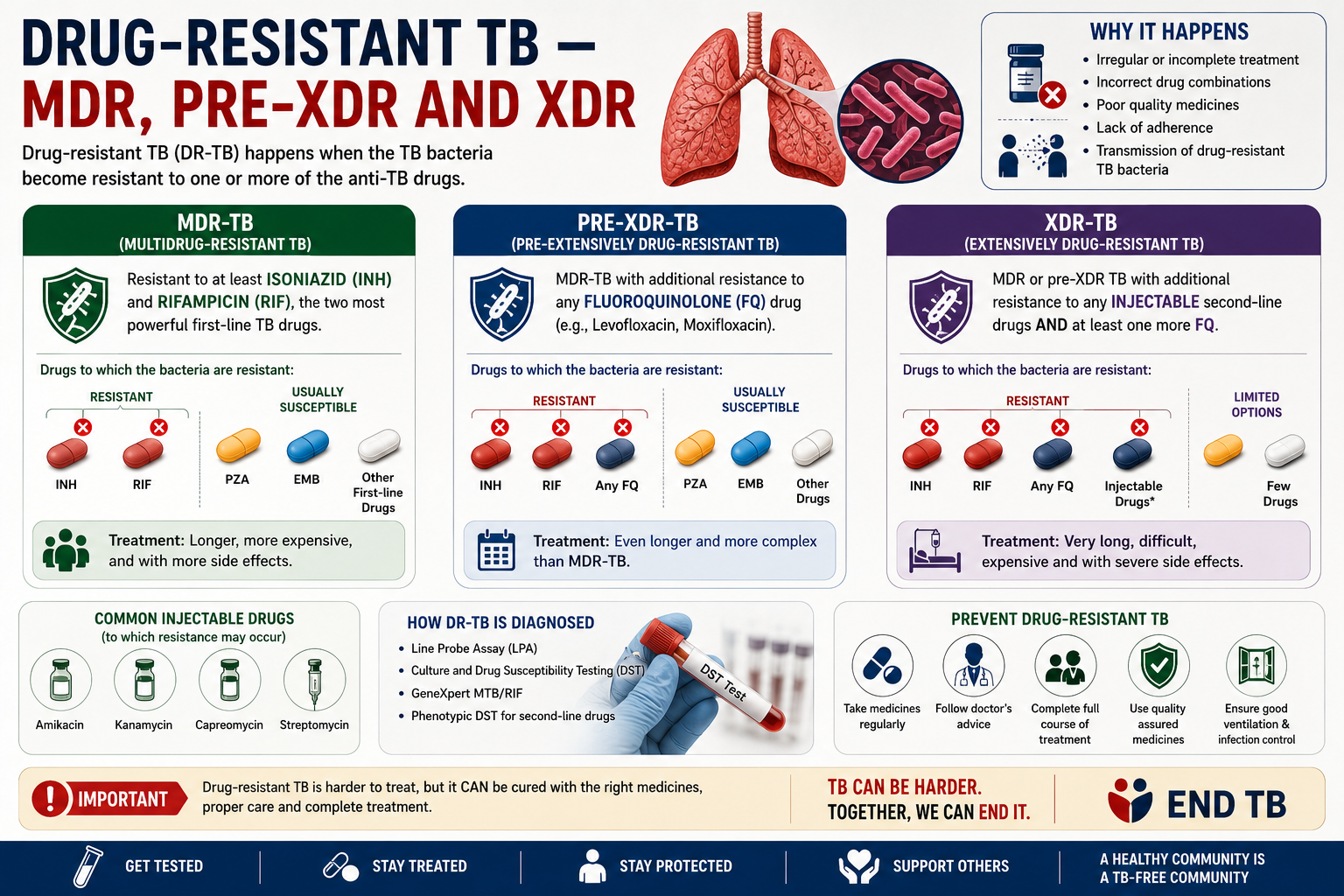
Drug-Resistant TB — MDR, Pre-XDR and XDR
Drug-resistant TB arises when M. tuberculosis develops resistance to first-line or second-line drugs — primarily due to incomplete treatment, incorrect regimens, or transmission from someone with resistant TB. India has one of the highest MDR-TB burdens globally: approximately 130,000 MDR-TB cases annually.
MDR-TB is resistant to at least Isoniazid and Rifampicin. Pre-XDR-TB adds fluoroquinolone resistance. XDR-TB is additionally resistant to Bedaquiline or Linezolid. All are treatable — but require longer, more complex regimens with more side effects. All DR-TB drugs are available free in India at government DR-TB centres under NTEP.
| Type | Definition | Duration | Core Drugs | Cure Rate | Free in India? |
|---|---|---|---|---|---|
| Drug-Sensitive TB | No resistance to first-line drugs | 6 months | HRZE then HR | 90%+ | Yes — all DOTS centres |
| MDR-TB | Resistant to Isoniazid + Rifampicin | 9–18 months | Bdq + Lfx + Lzd + Cfz + Z | 75–80% | Yes — DR-TB centres |
| Pre-XDR-TB | MDR + any fluoroquinolone resistance | 18–20 months | Bdq + Dlm + Lzd + Cfz | 65–75% | Yes — DR-TB centres |
| XDR-TB | MDR + FQ + Bdq or Lzd resistance | 6–24 months | BPaL (Bdq + Pa + Lzd) | 85%+ (BPaL) | Yes — selected centres |
| TB Meningitis | Standard DS-TB, CNS penetration needed | 9–12 months | HRZE then HR + steroids | 60–70% | Yes — NTEP |
| Spinal TB (Pott’s) | Standard DS-TB, bone penetration | 9–12 months | HRZE then HR ± surgery | 85%+ | Yes — NTEP |
HIV & TB Co-Infection — The Most Dangerous Combination
HIV destroys CD4 T-cells — the same immune cells that normally contain M. tuberculosis in a latent state. As CD4 count falls, the risk of TB reactivation rises dramatically. At CD4 below 200/mm³, TB can present atypically — with little or no cough, normal chest X-ray, and predominantly extrapulmonary disease that is easily missed.
Every person diagnosed with TB should be tested for HIV. Every person diagnosed with HIV should be screened for TB. The two infections require each other's testing as a standard of care — not an optional add-on.
Isoniazid Preventive Therapy (IPT)
All HIV-positive individuals without active TB should receive 6 months of isoniazid prophylaxis. This reduces the risk of developing TB by 33–60% and is standard practice at IID Hospital for every HIV patient.
Rifampicin-ART Drug Interactions
Rifampicin is a powerful enzyme inducer that significantly lowers levels of most NNRTI and PI-based ART drugs. The ART regimen must be adjusted — typically to efavirenz or dolutegravir-based regimen — when TB treatment is started.
Timing of ART Initiation
ART should be started within 2–8 weeks of starting TB treatment in most co-infected patients. Exception: TB meningitis — delay ART to 4–8 weeks to reduce IRIS risk. This timing decision requires specialist expertise.
IRIS (Immune Reconstitution Inflammatory Syndrome)
As the immune system recovers on ART, it can overreact to TB bacteria — causing paradoxical worsening of TB symptoms. This requires recognition and management. Do not stop ART or TB treatment.
Overlapping Drug Toxicities
Both TB drugs and ART can cause hepatotoxicity, peripheral neuropathy, and nausea. Managing both regimens simultaneously requires careful monitoring of liver function, kidney function, and blood counts at every visit.
New TB cases in India every year — the world’s highest national burden
India accounts for 28% of the world’s TB cases despite having only 18% of the world’s population. TB in India is driven by overcrowding, malnutrition, high HIV co-infection rates, and the rising burden of drug-resistant TB. Despite this, India’s national programme has made remarkable progress — new infections declined by 16% and TB deaths declined by 18% between 2015 and 2022.
What Is Free Under India’s NTEP Programme
What Patients Say About Dr. Pratik Savaj
I was coughing for three months and was told by two clinics it was a chest infection. Dr. Savaj ran GeneXpert and confirmed TB within 24 hours. He started DOTS immediately and supervised every month. Eight months later I am cured.
I had MDR-TB after failing first-line treatment elsewhere. Dr. Savaj designed a second-line regimen, managed every side effect, and coordinated with the district DOTS centre. Two years later I am culture-negative. The specialist difference was everything.
I was diagnosed with HIV and TB simultaneously. Dr. Savaj managed both conditions together — sequencing the treatment correctly, handling the drug interactions, and explaining every decision. Both are now controlled.
My company X-ray showed old TB scarring. Dr. Savaj explained latent TB clearly, started preventive isoniazid, and I completed the course with no active episode. His explanation removed months of anxiety.
My brother had TB and our whole family was worried. Dr. Savaj tested every household member, started preventive therapy where needed, and explained exactly how TB spreads. The right information made everything less frightening.
Six weeks of fever, night sweats, and weight loss — no diagnosis elsewhere. Dr. Savaj ran the right investigations, confirmed pulmonary TB, and started treatment the same day. Within four weeks I was feeling human again.
Frequently Asked Questions
About Tuberculosis
Answered by Dr. Pratik Savaj, FNB Infectious Diseases — IID Hospital, Vesu, Surat.